
There is no reliable method to prevent the development and progression of Alzheimer’s. There is no known cure for Alzheimer’s. The approaches that we have tried over the past 20-25 years have not prevented or inhibited the decline in cognitive function that is associated with Alzheimer’s.
Now, Professor Jan Aaseth (Norway) and Professor Urban Alehagen (Sweden) propose selenium supplementation as a prophylactic measure to inhibit the decline of cognitive function, especially in the selenium-poor regions of the world. They hypothesize that the optimal functioning of the selenoproteins SEPP, GPx, and TrxR is necessary to protect against the cognitive decline associated with Alzheimer’s disease.
There is a considerable amount of research in human studies that forms the basis for their recommendation.
Selenium and brain function
Adequate supply of selenium is crucial to cerebral functions. In cases of low selenium status, the brain selenium is maintained at the expense of selenium to other cells and tissues in the body.
The selenoprotein SEPP – the circulating selenium transporter – is the most important extracellular selenoprotein. It is the selenoprotein that delivers selenium to the brain and the neurons.
The selenoproteins GPx1 and GPx4 (glutathione peroxidases) and TrxR (thioredoxin reductases) are important intracellular antioxidants in the brain and the neurons.
Observational studies of selenium status and cognitive decline
Drs. Aaseth and Alehagen has amassed quite a bit of data from human studies that show an association between low selenium intakes and/or low selenium status and various aspects of cognitive decline.
Please remember, in reading about the studies summarized below, that researchers at the University of East Anglia, in the United Kingdom, have estimated that the most likely range for optimal functioning of selenoproteins is between 120 and 150 micrograms of selenium per liter of plasma [Hurst 2010].
- An Italian study with 1012 adults aged 65 or older showed lower coordination scores and lower mini mental state examination (MMSE) scores in individuals with selenium levels below 66.7 micrograms per liter as compared with individuals with selenium levels above 82.3 micrograms per liter.
- A French study of 1166 adults aged 60 – 70 years showed greater cognitive decline in individuals with selenium levels below 75.8 micrograms per liter as compared with individuals with selenium levels above 86.9 micrograms per liter. Furthermore, the French study showed that, over a nine-year period, decline in cognitive ability was associated with a decline in plasma selenium concentrations. As the amount of selenium available to the brain and the neurons went down, so too did the cognitive ability.
- A Chinese study of 2000 adults, 65 years or older, living in rural areas, showed an association between low nail selenium concentrations and low cognitive performance.
- A Spanish study showed lower serum selenium concentrations in patients with Alzheimer’s disease (mean: 121 micrograms per liter) than in mild cognitive impairment patients (mean: 127 micrograms per liter).
- A Dutch study showed lower selenium status in patients with very mild Alzheimer’s (82.2 micrograms per liter) versus healthy elderly adults (93.2 micrograms per liter).
Intervention studies of selenium and cognitive decline
There have been fewer intervention studies than observational studies, but the results are, if anything, more interesting.
- A French study of 4447 French participants aged 45 – 60 years who received a daily antioxidant cocktail including 100 micrograms of selenium for six years scored better on episodic memory, verbal memory, and executive functioning than did study participants who received a placebo treatment.
- A Dutch study of 225 Alzheimer’s drug-naïve patients who consumed a “medical food” containing 60 micrograms of selenium daily for 12 weeks showed significant improvement in a delayed verbal recall task as compared to patients taking a similar placebo.
- A Brazilian study of 31 older adults with mild cognitive impairment (MCI) assigned to consume one Brazil nut daily (an estimated intake of 288.75 micrograms of selenium per day) for 6 months showed improvement of selenium deficiency status and positive effects on some cognitive functions as compared to individuals in a control group.
- A Swedish study on which Dr. Alehagen was the principal investigator, the KiSel-10 study of 443 elderly home-living adults showed that daily supplementation with 200 micrograms of a high-selenium yeast preparation and with 200 milligrams of Coenzyme Q10 for four years resulted in significant improvements in health-related quality of life and vitality as well as in decreased levels of inflammation.
Selenium supplementation and cognitive decline in Alzheimer’s
Drs. Aaseth and Alehagen propose three mechanisms by which selenium supplementation to increase selenium status may be effective in countering the cognitive decline associated with Alzheimer’s disease.
It seems clear to them that neurodegeneration is related to low selenium and low Selenoprotein P (SEPP) levels.
- First, they suggest that SEPP selenoproteins form strong bonds with metals such as copper and iron. The SEPP binding with copper and iron could help to block the metal-mediated aggregation of beta¬-amyloid.
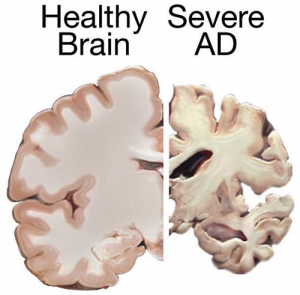
Remember: the clumping together of the beta-amyloid protein pieces is what forms the brain plaque characteristic of Alzheimer’s disease.
- Secondly, they suggest that selenium is necessary to prevent or inhibit the aggregation of tau proteins in the neurofibrillary tangles typical of Alzheimer’s disease.
- Thirdly, they address the intracellular antioxidant role of the GPx and TrxR selenoproteins. In this context, they point out that low selenium status means less SEPP selenoprotein to prevent beta-amyloid aggregation and that the trapping of the available SEPP selenoproteins by the beta-amyloid plaques means less selenium available for the antioxidant function of the GPx and TrxR selenoproteins.
Optimal selenoprotein levels necessary to avoid neurodegeneration
In many regions of the world, the daily intakes of selenium are not adequate to insure the optimal functioning of the selenoproteins. These selenoproteins are especially important to brain function and to the prevention of the development and progression of neurodegenerative diseases such as Alzheimer’s.
A pharmaceutical-grade organic high-selenium yeast supplement such as the one used in the KiSel-10 study may be part of the answer to the prevention of age-related diseases such as heart disease, cancer, and Alzheimer’s. Obviously, Alzheimer’s involves multiple biological pathways, but some of the important pathways require an adequate supply of selenium.
Sources
Aaseth, J., Alexander, J., Bjørklund, G., Hestad, K., Dusek, P., Roos, P. M., & Alehagen, U. (2016). Treatment strategies in Alzheimer’s disease: a review with focus on selenium supplementation. Biometals: An International Journal on The Role of Metal Ions in Biology, Biochemistry, and Medicine, 29(5), 827-839. doi:10.1007/s10534-016-9959-8
Alehagen, U., Alexander, J., & Aaseth, J. (2016). Supplementation with Selenium and Coenzyme Q10 Reduces Cardiovascular Mortality in Elderly with Low Selenium Status. A Secondary Analysis of a Randomised Clinical Trial. Plos One, 11(7), e0157541. doi:10.1371/journal.pone.0157541
Alehagen, U., Lindahl, T. L., Aaseth, J., Svensson, E., & Johansson, P. (2015). Levels of sP-selectin and hs-CRP Decrease with Dietary Intervention with Selenium and Coenzyme Q10 Combined: A Secondary Analysis of a Randomized Clinical Trial. Plos One, 10(9), e0137680. doi:10.1371/journal.pone.0137680
Hurst, R., Armah, C. N., Dainty, J. R., Hart, D. J., Teucher, B., Goldson, A. J., & Fairweather-Tait, S. J. (2010). Establishing optimal selenium status: results of a randomized, double-blind, placebo-controlled trial. The American Journal of Clinical Nutrition, 91(4), 923-931.
Johansson, P., Dahlström, Ö., Dahlström, U., & Alehagen, U. (2015). Improved Health-Related Quality of Life, and More Days out of Hospital with Supplementation with Selenium and Coenzyme Q10 Combined. Results from a Double Blind, Placebo-Controlled Prospective Study. The Journal of Nutrition, Health & Aging, 19(9), 870-877. doi:10.1007/s12603-015-0509-9
Disclaimer: The information presented in this review article is not intended as medical advice and should not be used as such.
One Reply to “Selenium and Alzheimer’s disease and cognitive decline”